Training and Assessment Delivered on Behalf of Allens Training Pty Ltd RTO 90909
The Ups and Downs of CPR
A Lifesaving Technique’s Journey Through Time
When I walked into the school gym and saw 50 or so manikins laid out in a grid, I had no idea what was going on! My teacher hadn’t really said much more than we were going to learn some first aid and didn’t particularly seem that interested. Turns out is was a CPR course!
Little did I know that I was about to have my first real exposure to a lifesaving skill that was going to follow me through my working life and end up being my career. All I could think of was “It’s cold in here, why didn’t I wear my Jumper!” More on that later.
What does CPR stand for?
CPR stands for Cardiopulmonary Resuscitation.
You can break that mouthful down into three key parts:
- Cardio – To do with the heart and circulation of blood around the body
- Pulmonary – to do with the lungs
- Resuscitation – trying to revive someone who is apparently dead
Together Cardiopulmonary Resuscitation is the process of a someone maintaining the circulation and oxygenation of a person who has suffered a cardiac arrest.
You can see why I prefer to write CPR!
Why was CPR invented?
Our bodies need oxygen to get to living cells so they can function and keep us alive. When a person stops breathing effectively, they need CPR to maintain their live until they can receive specialist medical attention.
CPR is our best practice technique for first responders to assist someone who has had a cardiac arrest. The best place to learn CPR is in a First Aid or CPR course.
In this post we’ll explore the history of CPR and see how it progressive invention and development led us to our current understanding of how a first responder can best help someone who is not responsive and not breathing. I think you’ll find it interesting.
Note: This is aimed at first aiders who are interested in learning more about the history of CPR. As such I’m focussing on making things as easy to understand as I can and avoid medical terminology as much as possible. If you want to get the juicy medical stuff, please see the references at the end of this post.
When was CPR invented? – Not as Recently as You’d Think!
Most people associate CPR and “Mouth to Mouth” as very recent inventions of modern medicine. But in fact the earliest references go back a long way in history and are closely linked to a person’s breathing.
Both the Bible and Ancient Egyptian literature talk about the Breath of Life in various ways. They even include Mouth to Mouth contact being used to assist in bringing someone back to life.
On a slightly more graphic note, it appears Greek surgeon Galen, who lived in the 2nd and 3rd centuries, used bellows to keep the lungs of animals inflated while he dissected them in attempt to learn how the heart works. There isn’t evidence he did this to keep them alive, but he must’ve been very close to working that out.
When did we start to make real progress in the invention of CPR?
We don’t really see any more thought put into this in Western Medicine until the Renaissance. Paulus Bagellardus, In Italian Physician during the 15th Century, literally wrote the book on medical care of Infants and Children. (“A little book about the illnesses of children”. The title doesn’t sound quite so whimsical in its Latin form – Libellus de egritudinibus infantium)
His book had advice to new mothers. He wrote that “if she finds [the baby] warm, not black, she should blow into its mouth, if it has no respiration.’ He was well ahead of it time compared to his contemporaries.
In 18th century, Physicians worked on the idea of restarting a dying person’s breathing. This work included the first, well documented case of what we would recognise at Resuscitation. This was the invention of modern mouth to mouth resuscitation or Artificial Respiration.
In 1732, in Scotland, a Coal miner named James Blair collapsed and apparently died. Surgeon William A. Tossach was called to the scene and used mouth-to-mouth resuscitation to resuscitate him, in front of nearly 400 people.
What about chest compressions? Surgeons had previously tried direct stimulation of the heart, but bystander chest compressions weren’t really encouraged. This was more the domain of the medical professional than bystanders or first responders and generally only attempted in a hospital setting.
Today, CPR is now a skill that’s essentially expected of a bystander, even with no medical background. So how did this go from a medical technique to a life skill. The answer starts to become clear in the 1960s.
So how CPR get to where we are today?
The first half of the 20th century saw a range of artificial breathing techniques tried. You can see a few of them in the picture below:
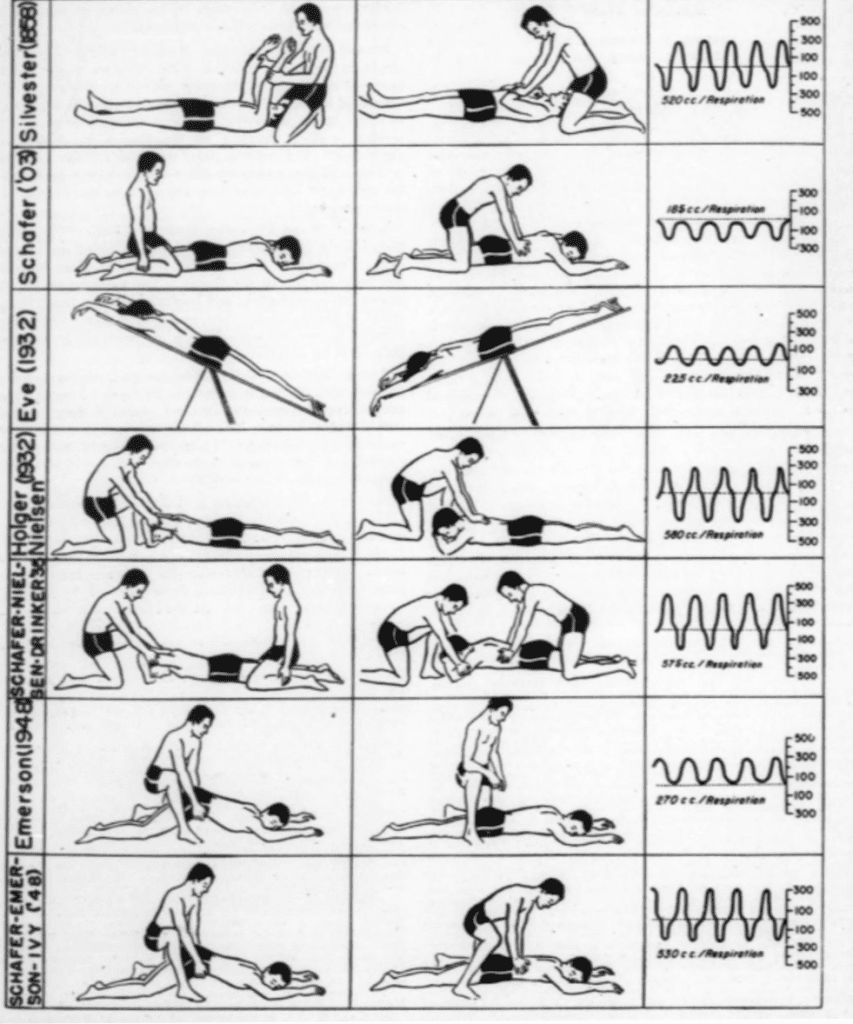
While this was great, the evidence was mounting that a combined approach of chest compression and artificial respiration was going to provide the best outcomes for a casualty. Doctors started compressing on a patient’s sternum to stimulate movement of blood around the body. The two techniques together are CPR. The push was on to teach this skill to doctors and surgeons.
But what about us, the non-doctors?
At first there was some resistance to teaching this technique to the public, despite the possible benefits. It seems this came mainly from a desire to ensure medical professionals are well trained in the technique first. Maybe a bit of “We don’t want you knowing something your physician doesn’t.”
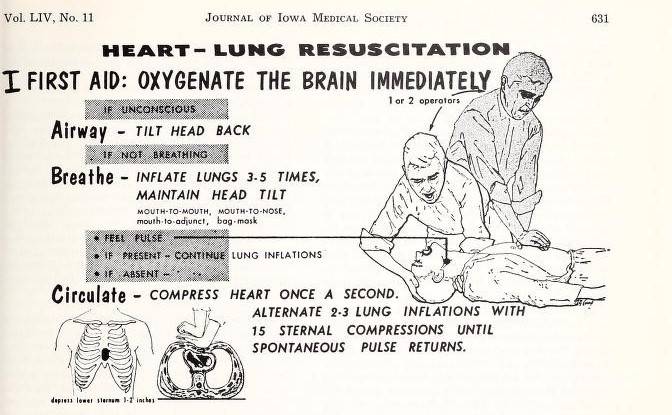
However, not everyone agreed. During this time there were still people producing training for non-medical professional. For example, “The pulse of life” was produced in 1962 as a training film, for doctors and everyday people alike.
While this wasn’t the first training film, it appears to be the first to use the sequence Airway-Breathing-Circulation to assist recall. An early version of A-B-C is pictured below. Todays DRSABCD started here.
One thing I find interesting is huge leaps have been made in the understanding of CPR in recent decades. We have a vastly improved understanding of what’s happening and CPR now provides the best balance between chest compression and rescue breaths. This means we get the best outcomes.
So how does it work today?
This includes specialised bodies from around the world cooperating to share research and come up with recommendations based on the best available evidence. The International liaison committee on resuscitation or ILCOR coordinates this around the world. It’s this cooperation that’s lead to some of the major recent changes:
- Standardising of CPR best practices such as 30 chest compressions to 2 rescue breaths.
- Fine tuning the factors that improve outcomes for casualties, such as concentrating on location, depth and rate of compressions.
- Improving the understanding of the role of defibrillation in Cardiac Arrest response
On a local level, two key organisations provide guidence on CPR and Emergency Response. The first is the Australian Resuscitation Council – They represent a wide range of medical stakeholders. They review information from around the world, including ILCOR, and make recommendations for how they apply within Australia.
The second body is ANZCOR or the Australian and New Zealand Council on Resuscitation. This combined body does what it says on the tin. It represents the joint interests of Australia and New Zealand and provides representation for the two countries with ILCOR.
These bodies look after two websites – resus.org.au and anzcor.org. These sites provide a great resource for trainers like me, when we get tricky or unusual questions such as “Why have we stopped doing mouth to mouth?” (Hint – The answer is we haven’t, we’re just a bit more careful about it now. More on that in a later post!)
Back to my High School Gym
All that leads to me, standing with my classmates in a freezing cold gym. I knew none of the above history and my instructor didn’t tell me either. I did learn a few things that day:
- Quick action can save someone’s life. Don’t wait, get help and get started!
- Don’t try and be perfect, but do the best you can, always reaching for the goal of best practice.
- A passionate instructor can make all the difference.
What I learnt that day stuck with me and meant that when I had the chance to become a CPR/First Aid instructor myself, I jumped at it. Not just because it was easier than laying timber floors, but because I had the chance to help someone save a life.
CPR has gone from an obscure byproduct of experimentation to a refined and effective technique that can be used by anyone.
Getting trained in CPR is practical and affordable for almost everyone.
Every person trained is a boost to someone’s chance of survival.
Will you be that person?
References and additional resources.
A. ARC – The Australian Resuscitation Council – Resus.org
B. ANZCOR – Australian and New Zealand Committee on Resuscitation Guidelines – anzcor.org
C. References
- Artificial Respiration – The history of an ideas By AB Baker, Medical History Volume XV Number 4 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1034194/
- https://ilcor.org/about
- https://resus.org.au/international-liaison-committee-resuscitation-ilcor/
- https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.106.610907
- https://archive.org/details/journalofiowamed54unse/page/628/mode/2up
Summary
The History and Invention of CPR
Cardiopulmonary Resuscitation (CPR) has evolved over centuries from ancient resuscitation concepts to the modern life-saving technique we know today.
- Ancient Origins: The earliest ideas of resuscitation date back to biblical times, with mentions of the “Breath of Life” and mouth-to-mouth techniques.
- Early Science: Early scientific explorations into resuscitation began as far back as the 2nd century, with studies on lung inflation.
- Modern Development: The first documented case of modern mouth-to-mouth resuscitation was in 1732. The 20th century saw the combination of chest compressions with artificial respiration, forming the basis of modern CPR.
- Public Training: By the 1960s, training films were created to teach the public the vital “Airway-Breathing-Circulation” sequence, making CPR a widespread and accessible skill.